














U-MSC Stem Cells Treatments
The Role of Regenerative Medicine in Autoimmune Disorders
By modulating the body’s immune response, regenerative medicine therapies offer a promising treatment option for individuals struggling with the disabling effects of autoimmune conditions.
Umbilical Cord-derived Mesenchymal Stem Cell Therapies
U-MSC is currently the most potent biologic available in the field of regenerative medicine.
This type of stem cell is a game-changer for treating autoimmune diseases, such as rheumatoid arthritis, lupus, and Crohn’s disease its potential is rooted in its capability to replace, repair, and rejuvenate damaged or malfunctioning cells within the body.
Are you facing challenges with autoimmune disorders?
Autoimmune disorders are defined by a dysregulated immune response wherein the body’s immunological system mistakenly identifies and assaults its own cellular constituents and tissues.
Such misdirected immune responses precipitate inflammation, often resulting in discomfort, pain, and potential tissue damage across multiple organ systems.
The underlying etiology of this self-reactivity remains a topic of extensive research. However, these disorders arise from a complex interplay of genetic, environmental, and immunological factors.

Anti-inflammatory and immunomodulatory effects of regenerative medicine
Umbilical cord mesenchymal stem cells (U-MSCs) and exosomes derived from these cells possess the capacity to modulate the body’s immune response through diverse mechanisms of action.
• Reduce the production of pro-inflammatory cytokines chemical messengers that promote inflammation.
• Promote the growth of T-regulatory cells a type of immune cell that helps keep the immune response in check.
• Transmit anti-inflammatory and immunomodulatory signals to immune cells.
U-MSC Stem Cells
Mesenchymal stem cells derived from the umbilical cord, possess a unique pluripotency that allows them to differentiate into various cell types. They can enhance the body’s intrinsic capacity for tissue repair and healing.
U-MSC Derived Exosomes
Exosomes are like little cellular packages that U-MSC stem cells release. They contain essential information in the form of proteins, lipids, and RNA that can guide the behavior of other cells.
Identifying autoimmune conditions responsive to U-MSC stem cell therapies
Rheumatoid Arthritis
Clinical evidence evidence suggests that U-MSCs can suppress the inflammatory responses characteristic of this condition, potentially leading to decreased joint destruction and inflammation.
Systemic Lupus Erythematosus (SLE)
Clinical studies indicate that the administration of U-MSCs can modulate aberrant immune responses in SLE, restoring a balance in immune function.
Crohn's Disease
The anti-inflammatory and tissue regenerative properties of U-MSCs have shown the potential to reduce inflammation and promote mucosal healing in patients with Crohn’s disease.
Multiple Sclerosis
There is emerging evidence suggesting that U-MSCs and exosomes can modulate the immune system, potentially leading to reduced neuroinflammation and promoting neural repair.
Psoriasis
Early studies show that U-MSCs may help regulate the immune system’s overactivity, which could alleviate skin inflammation and lesions in psoriatic patients.
Bačenkov, Darina; Trebuňová, Marianna; Morochovič, Radoslav; Dosedla, Erik; Balogová, Alena Findrik
Interaction between Mesenchymal Stem Cells and the Immune System in Rheumatoid Arthritis Journal Article
In: 2022.
@article{nokey,
title = {Interaction between Mesenchymal Stem Cells and the Immune System in Rheumatoid Arthritis},
author = {Darina Bačenkov and Marianna Trebuňová and Radoslav Morochovič and Erik Dosedla and Alena Findrik Balogová},
url = {https://doi.org/10.3390%2Fph15080941},
year = {2022},
date = {2022-08-15},
urldate = {2022-08-15},
abstract = {Rheumatoid arthritis (RA) is an autoimmune disease that causes damage to joints. This review focuses on the possibility of influencing the disease through immunomodulation by mesenchymal stem cells (MSCs). There is an occurrence of rheumatoid factor and RA-specific autoantibodies to citrullinated proteins in most patients. Citrulline proteins have been identified in the joints of RA patients, and are considered to be the most suitable candidates for the stimulation of anti-citrulline protein antibodies production. Fibroblast-like proliferating active synoviocytes actively promote inflammation and destruction in the RA joint, in association with pro-inflammatory cells. The inflammatory process may be suppressed by MSCs, which are a population of adherent cells with the following characteristic phenotype: CD105+, CD73+, CD90+, CD45−, CD34− and HLA DR−. Following the stimulation process, MSCs are capable of immunomodulatory action through the release of bioactive molecules, as well as direct contact with the cells of the immune system. Furthermore, MSCs show the ability to suppress natural killer cell activation and dendritic cells maturation, inhibit T cell proliferation and function, and induce T regulatory cell formation. MSCs produce factors that suppress inflammatory processes, such as PGE2, TGF-β, HLA-G5, IDO, and IL-10. These properties suggest that MSCs may affect and suppress the excessive inflammation that occurs in RA. The effect of MSCs on rheumatoid arthritis has been proven to be a suitable alternative treatment thanks to successful experiments and clinical studies.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Zeng, Liuting; Yu, Ganpeng; Yang, Kailin; Xiang, Wang; Li, Jun; Chen, Hua
Efficacy and Safety of Mesenchymal Stem Cell Transplantation in the Treatment of Autoimmune Disease Journal Article
In: 2022.
@article{nokey,
title = {Efficacy and Safety of Mesenchymal Stem Cell Transplantation in the Treatment of Autoimmune Disease},
author = {Liuting Zeng and Ganpeng Yu and Kailin Yang and Wang Xiang and Jun Li and Hua Chen},
url = {https://doi.org/10.1155%2F2022%2F9463314},
year = {2022},
date = {2022-03-24},
urldate = {2022-03-24},
abstract = {Autoimmune diseases are a series of diseases caused by the immune system's response to self-antigens, resulting in self-tissue damage or dysfunction. It mainly includes systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), Sjogren's syndrome, polymyositis and dermatomyositis. Many autoimmune diseases are characterized by the production of autoantibodies, which bind to the host's own proteins or form immune complexes and deposit in tissues. Any organ of the body may become a target organ for autoimmunity, including skin, joints, kidneys, and blood vessels. The inflammatory effect caused by autoantibodies is mediated by binding to Fc receptors on leukocytes, which is an important cause of downstream tissue damage. Meanwhile, autoantibodies can also directly mediate tissue damage in diseases through complement activation [5]. In the development stage of the disease, genetic factors and environmental factors may interact in turn to promote the development of autoimmunity and ultimately lead to tissue inflammation and damage, becoming a chronic disease with multiple organs and multiple system damage.
Clinically, once diagnosed, patients should be treated with medication in time to avoid further development of the disease causing damage to organs or systems such as the liver and kidney. Clinically, commonly used glucocorticoids and traditional disease-improving antirheumatic drugs (DMARDs) have good anti-inflammatory, pain-relieving, and improving or delaying disease progression effects and are still used as the first-line choice for clinical treatment of rheumatic immune diseases [9, 10]. However, for first-line treatments with single or combined regimens that do not respond well or cannot tolerate them, other treatment options with potential curative effects need to be considered . For example, stem cell transplantation, biological preparations, or new botanical preparations, as well as some antirheumatic drug candidates that may modulate or suppress immunity, in order to alleviate the condition of patients with refractory rheumatism and improve their quality of life. Among them, mesenchymal stem cells are one of the most promising therapeutic strategies },
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Clinically, once diagnosed, patients should be treated with medication in time to avoid further development of the disease causing damage to organs or systems such as the liver and kidney. Clinically, commonly used glucocorticoids and traditional disease-improving antirheumatic drugs (DMARDs) have good anti-inflammatory, pain-relieving, and improving or delaying disease progression effects and are still used as the first-line choice for clinical treatment of rheumatic immune diseases [9, 10]. However, for first-line treatments with single or combined regimens that do not respond well or cannot tolerate them, other treatment options with potential curative effects need to be considered . For example, stem cell transplantation, biological preparations, or new botanical preparations, as well as some antirheumatic drug candidates that may modulate or suppress immunity, in order to alleviate the condition of patients with refractory rheumatism and improve their quality of life. Among them, mesenchymal stem cells are one of the most promising therapeutic strategies
González, Lina María; Ospina, Laura Natalia; Sperling, Laura Elena; Chaparro, Orlando; Cucarián, Jaison Daniel
Therapeutic Effects of Physical Exercise and the Mesenchymal Stem Cell Secretome by Modulating Neuroinflammatory Response in Multiple Sclerosis Journal Article
In: 2022.
@article{nokey,
title = {Therapeutic Effects of Physical Exercise and the Mesenchymal Stem Cell Secretome by Modulating Neuroinflammatory Response in Multiple Sclerosis},
author = {Lina María González and Laura Natalia Ospina and Laura Elena Sperling and Orlando Chaparro and Jaison Daniel Cucarián},
url = {10.2174/1574888X16666211209155333},
year = {2022},
date = {2022-02-18},
abstract = {Multiple Sclerosis (MS) is a neurodegenerative, demyelinating, and chronic inflammatory disease characterized by Central Nervous System (CNS) lesions that lead to high levels of disability and severe physical and cognitive disturbances. Conventional therapies are not enough to control the neuroinflammatory process in MS and are not able to inhibit ongoing damage to the CNS. Thus, the secretome of mesenchymal stem cells (MSC-S) has been postulated as a potential therapy that could mitigate symptoms and disease progression. We considered that its combination with physical exercise (EX) could induce superior effects and increase the MSC-S effectiveness in this condition. Recent studies have revealed that both EX and MSC-S share similar mechanisms of action that mitigate auto-reactive T cell infiltration, regulate the local inflammatory response, modulate the proinflammatory profile of glial cells, and reduce neuronal damage. Clinical and experimental studies have reported that these treatments in an isolated way also improve myelination, regeneration, promote the release of neurotrophic factors, and increase the recruitment of endogenous stem cells. Together, these effects reduce disease progression and improve patient functionality. Despite these results, the combination of these methods has not yet been studied in MS. In this review, we focus on molecular elements and cellular responses induced by these treatments in a separate way, showing their beneficial effects in the control of symptoms and disease progression in MS, as well as indicating their contribution in clinical fields. In addition, we propose the combined use of EX and MSC-S as a strategy to boost their reparative and immunomodulatory effects in this condition, combining their benefits on synaptogenesis, neurogenesis, remyelination, and neuroinflammatory response. The findings here reported are based on the scientific evidence and our professional experience that will bring significant progress to regenerative medicine to deal with this condition.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Sarsenova, Madina; Issabekova, Assel; Abisheva, Saule; Rutskaya-Moroshan, Kristina; Ogay, Vyacheslav; Saparov, Arman
Mesenchymal Stem Cell-Based Therapy for Rheumatoid Arthritis Journal Article
In: 2021.
@article{nokey,
title = {Mesenchymal Stem Cell-Based Therapy for Rheumatoid Arthritis},
author = {Madina Sarsenova and Assel Issabekova and Saule Abisheva and Kristina Rutskaya-Moroshan and Vyacheslav Ogay and Arman Saparov},
url = {https://doi.org/10.3390%2Fijms222111592},
year = {2021},
date = {2021-11-22},
abstract = {Mesenchymal stem cells (MSCs) have great potential to differentiate into various types of cells, including but not limited to, adipocytes, chondrocytes and osteoblasts. In addition to their progenitor characteristics, MSCs hold unique immunomodulatory properties that provide new opportunities in the treatment of autoimmune diseases, and can serve as a promising tool in stem cell-based therapy. Rheumatoid arthritis (RA) is a chronic systemic autoimmune disorder that deteriorates quality and function of the synovium membrane, resulting in chronic inflammation, pain and progressive cartilage and bone destruction. The mechanism of RA pathogenesis is associated with dysregulation of innate and adaptive immunity. Current conventional treatments by steroid drugs, antirheumatic drugs and biological agents are being applied in clinical practice. However, long-term use of these drugs causes side effects, and some RA patients may acquire resistance to these drugs. In this regard, recently investigated MSC-based therapy is considered as a promising approach in RA treatment. In this study, we review conventional and modern treatment approaches, such as MSC-based therapy through the understanding of the link between MSCs and the innate and adaptive immune systems. Moreover, we discuss recent achievements in preclinical and clinical studies as well as various strategies for the enhancement of MSC immunoregulatory properties.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Shen, Ziwei; Huang, Wei; Liu, Jun; Tian, Jie; Wang, Shengjun; Rui, Ke
Effects of Mesenchymal Stem Cell-Derived Exosomes on Autoimmune Diseases Journal Article
In: 2021.
@article{nokey,
title = {Effects of Mesenchymal Stem Cell-Derived Exosomes on Autoimmune Diseases},
author = {Ziwei Shen and Wei Huang and Jun Liu and Jie Tian and Shengjun Wang and Ke Rui},
url = {https://doi.org/10.3389/fimmu.2021.749192},
year = {2021},
date = {2021-09-21},
urldate = {2021-09-21},
abstract = {Recent years, the immunosuppressive properties of mesenchymal stem cells (MSCs) have been demonstrated in preclinical studies and trials of inflammatory and autoimmune diseases. Emerging evidence indicates that the immunomodulatory effect of MSCs is primarily attributed to the paracrine pathway. As one of the key paracrine effectors, mesenchymal stem cell-derived exosomes (MSC-EXOs) are small vesicles 30-200 nm in diameter that play an important role in cell-to-cell communication by carrying bioactive substances from parental cells. Recent studies support the finding that MSC-EXOs have an obvious inhibitory effect toward different effector cells involved in the innate and adaptive immune response. Moreover, substantial progress has been made in the treatment of autoimmune diseases, including multiple sclerosis (MS), systemic lupus erythematosus (SLE), type-1 diabetes (T1DM), uveitis, rheumatoid arthritis (RA), and inflammatory bowel disease (IBD). MSC-EXOs are capable of reproducing MSC function and overcoming the limitations of traditional cell therapy. Therefore, using MSC-EXOs instead of MSCs to treat autoimmune diseases appears to be a promising cell-free treatment strategy. In this review, we review the current understanding of MSC-EXOs and discuss the regulatory role of MSC-EXOs on immune cells and its potential application in autoimmune diseases.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Hwang, Joel Jihwan; Rim, Yeri Alice; Nam, Yoojun; Ju, Ji Hyeon
Recent Developments in Clinical Applications of Mesenchymal Stem Cells in the Treatment of Rheumatoid Arthritis and Osteoarthritis Journal Article
In: 2021.
@article{nokey,
title = {Recent Developments in Clinical Applications of Mesenchymal Stem Cells in the Treatment of Rheumatoid Arthritis and Osteoarthritis},
author = {Joel Jihwan Hwang and Yeri Alice Rim and Yoojun Nam and Ji Hyeon Ju},
url = {https://doi.org/10.3389%2Ffimmu.2021.631291},
year = {2021},
date = {2021-03-08},
urldate = {2021-03-08},
abstract = {Mesenchymal stem cell (MSC) therapies have been used as cell-based treatments for decades, owing to their anti-inflammatory, immunomodulatory, and regenerative properties. With high expectations, many ongoing clinical trials are investigating the safety and efficacy of MSC therapies to treat arthritic diseases. Studies on osteoarthritis (OA) have shown positive clinical outcomes, with improved joint function, pain level, and quality of life. In addition, few clinical MSC trials conducted on rheumatoid arthritis (RA) patients have also displayed some optimistic outlook. The largely positive outcomes in clinical trials without severe side effects establish MSCs as promising tools for arthritis treatment. However, further research is required to investigate its applicability in clinical settings. This review discusses the most recent advances in clinical studies on MSC therapies for OA and RA.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
El-Jawhari, Jehan J.; El-Sherbiny, Yasser; McGonagle, Dennis; Jones, Elena
In: 2021.
@article{nokey,
title = {Multipotent Mesenchymal Stromal Cells in Rheumatoid Arthritis and Systemic Lupus Erythematosus; From a Leading Role in Pathogenesis to Potential Therapeutic Saviors?},
author = {Jehan J. El-Jawhari and Yasser El-Sherbiny and Dennis McGonagle and Elena Jones},
url = {https://doi.org/10.3389%2Ffimmu.2021.643170},
year = {2021},
date = {2021-02-24},
urldate = {2021-02-24},
abstract = {The pathogenesis of the autoimmune rheumatological diseases including rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) is complex with the involvement of several immune cell populations spanning both innate and adaptive immunity including different T-lymphocyte subsets and monocyte/macrophage lineage cells. Despite therapeutic advances in RA and SLE, some patients have persistent and stubbornly refractory disease. Herein, we discuss stromal cells' dual role, including multipotent mesenchymal stromal cells (MSCs) also used to be known as mesenchymal stem cells as potential protagonists in RA and SLE pathology and as potential therapeutic vehicles. Joint MSCs from different niches may exhibit prominent pro-inflammatory effects in experimental RA models directly contributing to cartilage damage. These stromal cells may also be key regulators of the immune system in SLE. Despite these pro-inflammatory roles, MSCs may be immunomodulatory and have potential therapeutic value to modulate immune responses favorably in these autoimmune conditions. In this review, the complex role and interactions between MSCs and the haematopoietically derived immune cells in RA and SLE are discussed. The harnessing of MSC immunomodulatory effects by contact-dependent and independent mechanisms, including MSC secretome and extracellular vesicles, is discussed in relation to RA and SLE considering the stromal immune microenvironment in the diseased joints. Data from translational studies employing MSC infusion therapy against inflammation in other settings are contextualized relative to the rheumatological setting. Although safety and proof of concept studies exist in RA and SLE supporting experimental and laboratory data, robust phase 3 clinical trial data in therapy-resistant RA and SLE is still lacking.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Petrou, Panayiota; Kassis, Ibrahim; Levin, Netta; Paul, Friedemann; Backner, Yael; Benoliel, Tal; Oertel, Frederike Cosima
Beneficial effects of autologous mesenchymal stem cell transplantation in active progressive multiple sclerosis Journal Article
In: 2020.
@article{nokey,
title = {Beneficial effects of autologous mesenchymal stem cell transplantation in active progressive multiple sclerosis},
author = {Panayiota Petrou and Ibrahim Kassis and Netta Levin and Friedemann Paul and Yael Backner and Tal Benoliel and Frederike Cosima Oertel},
url = {https://doi.org/10.1093/brain/awaa333},
year = {2020},
date = {2020-12-01},
urldate = {2020-12-01},
abstract = {In this study (trial registration: NCT02166021), we aimed to evaluate the optimal way of administration, the safety and the clinical efficacy of mesenchymal stem cell (MSC) transplantation in patients with active and progressive multiple sclerosis. Forty-eight patients (28 males and 20 females) with progressive multiple sclerosis (Expanded Disability Status Scale: 3.0-6.5, mean : 5.6 ± 0.8, mean age: 47.5 ± 12.3) and evidence of either clinical worsening or activity during the previous year, were enrolled (between 2015 and 2018). Patients were randomized into three groups and treated intrathecally (IT) or intravenously (IV) with autologous MSCs (1 × 106/kg) or sham injections. After 6 months, half of the patients from the MSC-IT and MSC-IV groups were retreated with MSCs, and the other half with sham injections. Patients initially assigned to sham treatment were divided into two subgroups and treated with either MSC-IT or MSC-IV. The study duration was 14 months. No serious treatment-related safety issues were detected. Significantly fewer patients experienced treatment failure in the MSC-IT and MSC-IV groups compared with those in the sham-treated group (6.7%, 9.7%, and 41.9%, respectively, P = 0.0003 and P = 0.0008). During the 1-year follow-up, 58.6% and 40.6% of patients treated with MSC-IT and MSC-IV, respectively, exhibited no evidence of disease activity compared with 9.7% in the sham-treated group (P < 0.0001 and P < 0.0048, respectively). MSC-IT transplantation induced additional benefits on the relapse rate, on the monthly changes of the T2 lesion load on MRI, and on the timed 25-foot walking test, 9-hole peg test, optical coherence tomography, functional MRI and cognitive tests. Treatment with MSCs was well-tolerated in progressive multiple sclerosis and induced short-term beneficial effects regarding the primary end points, especially in the patients with active disease. The intrathecal administration was more efficacious than the intravenous in several parameters of the disease. A phase III trial is warranted to confirm these findings.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Lopez-Santalla, Mercedes; Fernandez-Perez, Raquel; Garin, Marina I.
Mesenchymal Stem/Stromal Cells for Rheumatoid Arthritis Treatment: An Update on Clinical Applications Journal Article
In: 2020.
@article{nokey,
title = {Mesenchymal Stem/Stromal Cells for Rheumatoid Arthritis Treatment: An Update on Clinical Applications},
author = {Mercedes Lopez-Santalla and Raquel Fernandez-Perez and Marina I. Garin},
url = {https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7465092/#:~:text=10.3390/cells9081852},
year = {2020},
date = {2020-08-09},
abstract = {Rheumatoid arthritis (RA) is a chronic systemic autoimmune disease that affects the lining of the synovial joints leading to stiffness, pain, inflammation, loss of mobility, and erosion of joints. Its pathogenesis is related to aberrant immune responses against the synovium. Dysfunction of innate and adaptive immunity, including dysregulated cytokine networks and immune complex-mediated complement activation, are involved in the progression of RA. At present, drug treatments, including corticosteroids, antirheumatic drugs, and biological agents, are used in order to modulate the altered immune responses. Chronic use of these drugs may cause adverse effects to a significant number of RA patients. Additionally, some RA patients are resistant to these therapies. In recent years, mesenchymal stem/stromal cell (MSCs)-based therapies have been largely proposed as a novel and promising stem cell therapeutic approach in the treatment of RA. MSCs are multipotent progenitor cells that have immunomodulatory properties and can be obtained and expanded easily. Today, nearly one hundred studies in preclinical models of RA have shown promising trends for clinical application. Proof-of-concept clinical studies have demonstrated satisfactory safety profile of MSC therapy in RA patients. The present review discusses MSC-based therapy approaches with a focus on published clinical data, as well as on clinical trials, for treatment of RA that are currently underway.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Wang, Liming; Huang, Shigao; Li, Shimei; Li, Ming; Shi, Jun; Bai, Wen; Wang, Qianyun; Zheng, Libo; Liu, Yongjun
Efficacy and Safety of Umbilical Cord Mesenchymal Stem Cell Therapy for Rheumatoid Arthritis Patients: A Prospective Phase I/II Study Journal Article
In: 2019.
@article{nokey,
title = {Efficacy and Safety of Umbilical Cord Mesenchymal Stem Cell Therapy for Rheumatoid Arthritis Patients: A Prospective Phase I/II Study},
author = {Liming Wang and Shigao Huang and Shimei Li and Ming Li and Jun Shi and Wen Bai and Qianyun Wang and Libo Zheng and Yongjun Liu},
url = {https://doi.org/10.2147%2FDDDT.S225613},
year = {2019},
date = {2019-12-19},
urldate = {2019-12-19},
abstract = {Rheumatoid arthritis (RA) is a chronic, autoimmune disease affecting multiple joints symmetrically.1 The main symptoms at the early stage of the disease are joint pain and swelling; at late stage, arthritis leads to joint stiffness, malformation, loss of function, and even disability.2 Currently, available medication for RA treatment has limited efficacy, including non-steroidal anti-inflammatory drugs (NSAIDs), disease-modifying anti-rheumatic drugs (DMARDs) and immunosuppressants.3 The target cytokine therapy has some therapeutic effects but without significant repair of injured joints, which restricts its widespread clinical use.
Mesenchymal stem cells (MSCs) are characterized by their regenerative property to repair parenchymal tissue and organs through differentiating into lineages of mesenchymal tissues, as well as immunomodulation.4 Injected MSCs can migrate to injured tissues and facilitate the recovery of damaged cells.5 Clinical studies have demonstrated the clinical benefits of MSCs in RA therapy.6 However, the therapeutic benefits of umbilical cord tissue-derived MSCs (UC-MSCs) for the treatment of RA have not been well studied clinically. As is known that the key factor in the pathogenesis of RA is the elevated cytokines arising from numerous synovial cells.7 MSCs can express various receptors for pro-inflammatory cytokines8 to reduce inflammation in RA patients. We have previously reported the safety and efficacy of UC-MSC for the treatment of RA patients for up to 8 months after UC-MSC infusion.9 The aim of this 3-year cohort study is to assess the long-term efficacy and safety of UC-MSC plus DMARDs therapy for RA. The data demonstrated that UC-MSC treatment was safe and able to benefit RA patients in long term when combined with DMARDs. Continuous UC-MSC treatment can resume patients’ physical activity function to achieve excellent clinical benefits.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Mesenchymal stem cells (MSCs) are characterized by their regenerative property to repair parenchymal tissue and organs through differentiating into lineages of mesenchymal tissues, as well as immunomodulation.4 Injected MSCs can migrate to injured tissues and facilitate the recovery of damaged cells.5 Clinical studies have demonstrated the clinical benefits of MSCs in RA therapy.6 However, the therapeutic benefits of umbilical cord tissue-derived MSCs (UC-MSCs) for the treatment of RA have not been well studied clinically. As is known that the key factor in the pathogenesis of RA is the elevated cytokines arising from numerous synovial cells.7 MSCs can express various receptors for pro-inflammatory cytokines8 to reduce inflammation in RA patients. We have previously reported the safety and efficacy of UC-MSC for the treatment of RA patients for up to 8 months after UC-MSC infusion.9 The aim of this 3-year cohort study is to assess the long-term efficacy and safety of UC-MSC plus DMARDs therapy for RA. The data demonstrated that UC-MSC treatment was safe and able to benefit RA patients in long term when combined with DMARDs. Continuous UC-MSC treatment can resume patients’ physical activity function to achieve excellent clinical benefits.
Genc, Bilgesu; Bozan, Hemdem Rodi; Genc, Sermin; Genc, Kursad
Stem Cell Therapy for Multiple Sclerosis Journal Article
In: 2018.
@article{nokey,
title = {Stem Cell Therapy for Multiple Sclerosis},
author = {Bilgesu Genc and Hemdem Rodi Bozan and Sermin Genc and Kursad Genc},
url = {https://dx.doi.org/10.1007/5584_2018_247},
year = {2018},
date = {2018-07-24},
abstract = {Multiple sclerosis (MS) is a chronic inflammatory, autoimmune, and neurodegenerative disease of the central nervous system (CNS). It is characterized by demyelination and neuronal loss that is induced by attack of autoreactive T cells to the myelin sheath and endogenous remyelination failure, eventually leading to functional neurological disability. Although recent evidence suggests that MS relapses are induced by environmental and exogenous triggers such as viral infections in a genetic background, its very complex pathogenesis is not completely understood. Therefore, the efficiency of current immunosuppression-based therapies of MS is too low, and emerging disease-modifying immunomodulatory agents such as fingolimod and dimethyl fumarate cannot stop progressive neurodegenerative process. Thus, the cell replacement therapy approach that aims to overcome neuronal cell loss and remyelination failure and to increase endogenous myelin repair capacity is considered as an alternative treatment option. A wide variety of preclinical studies, using experimental autoimmune encephalomyelitis model of MS, have recently shown that grafted cells with different origins including mesenchymal stem cells (MSCs), neural precursor and stem cells, and induced-pluripotent stem cells have the ability to repair CNS lesions and to recover functional neurological deficits. The results of ongoing autologous hematopoietic stem cell therapy studies, with the advantage of peripheral administration to the patients, have suggested that cell replacement therapy is also a feasible option for immunomodulatory treatment of MS. In this chapter, we overview cell sources and applications of the stem cell therapy for treatment of MS. We also discuss challenges including those associated with administration route, immune responses to grafted cells, integration of these cells to existing neural circuits, and risk of tumor growth. Finally, future prospects of stem cell therapy for MS are addressed.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Franceschetti, Tiziana; Bari, Cosimo De
The potential role of adult stem cells in the management of the rheumatic diseases Journal Article
In: 2017.
@article{nokey,
title = {The potential role of adult stem cells in the management of the rheumatic diseases},
author = {Tiziana Franceschetti and Cosimo De Bari},
url = {https://doi.org/10.1177%2F1759720X17704639},
year = {2017},
date = {2017-04-20},
urldate = {2017-04-20},
abstract = {Adult stem cells are considered as appealing therapeutic candidates for inflammatory and degenerative musculoskeletal diseases. A large body of preclinical research has contributed to describing their immune-modulating properties and regenerative potential. Additionally, increasing evidence suggests that stem cell differentiation and function are disrupted in the pathogenesis of rheumatic diseases. Clinical studies have been limited, for the most part, to the application of adult stem cell-based treatments on small numbers of patients or as a ‘salvage’ therapy in life-threatening disease cases. Nevertheless, these preliminary studies indicate that adult stem cells are promising tools for the long-term treatment of rheumatic diseases. This review highlights recent knowledge acquired in the fields of hematopoietic and mesenchymal stem cell therapy for the management of systemic sclerosis (SSc), systemic lupus erythematosus (SLE), rheumatoid arthritis (RA) and osteoarthritis (OA) and the potential mechanisms mediating their function.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Ennis, William J.; Sui, Audrey; Bartholomew, Amelia
Stem Cells and Healing: Impact on Inflammation Journal Article
In: 2013.
@article{nokey,
title = {Stem Cells and Healing: Impact on Inflammation},
author = {William J. Ennis and Audrey Sui and Amelia Bartholomew},
url = {https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3842880/},
year = {2013},
date = {2013-09-02},
abstract = {Significance
The number of patients with nonhealing wounds has rapidly accelerated over the past 10 years in both the United States and worldwide. Some causative factors at the macro level include an aging population, epidemic numbers of obese and diabetic patients, and an increasing number of surgical procedures. At the micro level, chronic inflammation is a consistent finding.
Recent Advances
A number of treatment modalities are currently used to accelerate wound healing, including energy-based modalities, scaffoldings, the use of mechano-transduction, cytokines/growth factors, and cell-based therapies. The use of stem cell therapy has been hypothesized as a potentially useful adjunct for nonhealing wounds. Specifically, mesenchymal stem cells (MSCs) have been shown to improve wound healing in several studies. Immune modulating properties of MSCs have made them attractive treatment options.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
The number of patients with nonhealing wounds has rapidly accelerated over the past 10 years in both the United States and worldwide. Some causative factors at the macro level include an aging population, epidemic numbers of obese and diabetic patients, and an increasing number of surgical procedures. At the micro level, chronic inflammation is a consistent finding.
Recent Advances
A number of treatment modalities are currently used to accelerate wound healing, including energy-based modalities, scaffoldings, the use of mechano-transduction, cytokines/growth factors, and cell-based therapies. The use of stem cell therapy has been hypothesized as a potentially useful adjunct for nonhealing wounds. Specifically, mesenchymal stem cells (MSCs) have been shown to improve wound healing in several studies. Immune modulating properties of MSCs have made them attractive treatment options.
Lihua Wang Liming Wang, Xiuli Cong
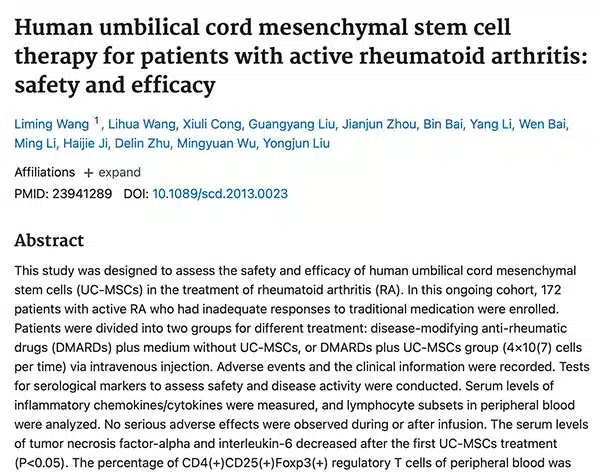
Human umbilical cord mesenchymal stem cell therapy for patients with active rheumatoid arthritis: safety and efficacy Journal Article
In: 2013.
@article{,
title = {Human umbilical cord mesenchymal stem cell therapy for patients with active rheumatoid arthritis: safety and efficacy},
author = {Liming Wang , Lihua Wang, Xiuli Cong, Guangyang Liu, Jianjun Zhou, Bin Bai, Yang Li, Wen Bai, Ming Li, Haijie Ji, Delin Zhu, Mingyuan Wu, Yongjun Liu},
url = {https://doi.org/10.1089/scd.2013.0023},
year = {2013},
date = {2013-08-13},
urldate = {2013-08-13},
abstract = {This study was designed to assess the safety and efficacy of human umbilical cord mesenchymal stem cells (UC-MSCs) in the treatment of rheumatoid arthritis (RA). In this ongoing cohort, 172 patients with active RA who had inadequate responses to traditional medication were enrolled. Patients were divided into two groups for different treatment: disease-modifying anti-rheumatic drugs (DMARDs) plus medium without UC-MSCs, or DMARDs plus UC-MSCs group (4×107 cells per time) via intravenous injection. Adverse events and the clinical information were recorded. Tests for serological markers to assess safety and disease activity were conducted. Serum levels of inflammatory chemokines/cytokines were measured, and lymphocyte subsets in peripheral blood were analyzed. No serious adverse effects were observed during or after infusion. The serum levels of tumor necrosis factor-alpha and interleukin-6 decreased after the first UC-MSCs treatment (P<0.05). The percentage of CD4+CD25+Foxp3+ regulatory T cells of peripheral blood was increased (P<0.05). The treatment induced a significant remission of disease according to the American College of Rheumatology improvement criteria, the 28-joint disease activity score, and the Health Assessment Questionnaire. The therapeutic effects maintained for 3–6 months without continuous administration, correlating with the increased percentage of regulatory T cells of peripheral blood. Repeated infusion after this period can enhance the therapeutic efficacy. In comparison, there were no such benefits observed in control group of DMARDS plus medium without UC-MSCs. Thus, our data indicate that treatment with DMARDs plus UC-MSCs may provide safe, significant, and persistent clinical benefits for patients with active RA.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Liu, Yanying; Mu, Rong; Wang, Shiyao; Long,; Liu, Xia
Therapeutic potential of human umbilical cord mesenchymal stem cells in the treatment of rheumatoid arthritis Journal Article
In: 2010.
@article{nokey,
title = {Therapeutic potential of human umbilical cord mesenchymal stem cells in the treatment of rheumatoid arthritis},
author = {Yanying Liu and Rong Mu and Shiyao Wang and Long and Xia Liu},
url = {https://doi.org/10.1186%2Far3187},
year = {2010},
date = {2010-11-16},
urldate = {2010-11-16},
abstract = {Rheumatoid arthritis (RA) is a chronic and systemic disease that primarily attacks synovial joints, leading to articular destruction and functional disability. RA imparts a massive burden on health services worldwide. Efforts to discover new target therapies have achieved considerable success. For instance, TNF-α inhibitors and B-cell-depleting therapies have benefited many RA patients [1,2]. However, these approaches are expensive and none of the currently widely used biological agents reaches longterm drug-free remission [3,4]. Therefore, it is important to develop new and more effective therapy for RA.
In RA, proinflammatory cytokines, such as TNF-α, IL-6, IL-1β and IL-17, play dominant pathological roles. Aberrant T help cells (Th) 17 and Th1 responses have been linked to pathogenesis of RA [5-7]. Furthermore, evidence is accumulating that a defect in number or function of regular T cells (Tregs) is important in the immune imbalance that culminates in RA [8,9]. The fibroblast-like synoviocytes (FLSs) are resident cells of synovial joints, involved in pannus formation, and are key players in the destruction of cartilage and bone in RA joint [10]. The ability of FLSs to stimulate both inflammation and tissue damage suggests that this cell type may be another critical target for the treatment of inflammatory arthritis [11].
Mesenchymal stem cells (MSCs) are cells of stromal origin that can exert profound immunosuppression by modulating T and B cell proliferation and differentiation, dendritic cell maturation and NK activity. These immunoregulatory properties encouraged a possible use of these cells to modulate autoimmune responses and in the treatment of autoimmue diseases [12,13]. To date, the experience of MSCs in the treatment of RA is limited to a few cases, with controversial results from preclinical models [14-18]. As of yet, the most common source of MSCs has been bone marrow. However, aspirating bone marrow is an invasive procedure. In addition, the number and the differentiating potential of bone marrow MSCs (BM-MSCs) decrease with age [19,20]. In contrast, the umbilical cord is a postnatal organ discarded after birth. The collection of umbilical cord MSCs (UC-MSCs) does not require any invasive procedure. In addition to the well-documented self-renewal and multipotent differentiation properties, UC-MSCs possess immunoregulatory capacities that have been permissive to allogeneic transplantation [21]. Given these characteristics, particularly the plasticity and developmental flexibility, the UC-MSCs are now considered an alternative source of stem cells and deserve to be examined in long-term clinical trials [22]. However, very little is known about UC-MSCs, and of note, there has been no report about UC-MSCs in the treatment of RA.
In this study, we reported our findings of the suppressive effect of UC-MSCs on the proliferation, invasive behavior and inflammatory responses of FLSs from RA patients. We also demonstrated that UC-MSCs could inhibit activation of T cells and induced Tregs expression in RA. More importantly, in mice, systemic infusion of UC-MSCs significantly reduced the severity of collagen-induced arthritis (CIA). In addition, the possible mechanism(s) underlying the UC-MSCs-mediated inhibitory effect were explored.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
In RA, proinflammatory cytokines, such as TNF-α, IL-6, IL-1β and IL-17, play dominant pathological roles. Aberrant T help cells (Th) 17 and Th1 responses have been linked to pathogenesis of RA [5-7]. Furthermore, evidence is accumulating that a defect in number or function of regular T cells (Tregs) is important in the immune imbalance that culminates in RA [8,9]. The fibroblast-like synoviocytes (FLSs) are resident cells of synovial joints, involved in pannus formation, and are key players in the destruction of cartilage and bone in RA joint [10]. The ability of FLSs to stimulate both inflammation and tissue damage suggests that this cell type may be another critical target for the treatment of inflammatory arthritis [11].
Mesenchymal stem cells (MSCs) are cells of stromal origin that can exert profound immunosuppression by modulating T and B cell proliferation and differentiation, dendritic cell maturation and NK activity. These immunoregulatory properties encouraged a possible use of these cells to modulate autoimmune responses and in the treatment of autoimmue diseases [12,13]. To date, the experience of MSCs in the treatment of RA is limited to a few cases, with controversial results from preclinical models [14-18]. As of yet, the most common source of MSCs has been bone marrow. However, aspirating bone marrow is an invasive procedure. In addition, the number and the differentiating potential of bone marrow MSCs (BM-MSCs) decrease with age [19,20]. In contrast, the umbilical cord is a postnatal organ discarded after birth. The collection of umbilical cord MSCs (UC-MSCs) does not require any invasive procedure. In addition to the well-documented self-renewal and multipotent differentiation properties, UC-MSCs possess immunoregulatory capacities that have been permissive to allogeneic transplantation [21]. Given these characteristics, particularly the plasticity and developmental flexibility, the UC-MSCs are now considered an alternative source of stem cells and deserve to be examined in long-term clinical trials [22]. However, very little is known about UC-MSCs, and of note, there has been no report about UC-MSCs in the treatment of RA.
In this study, we reported our findings of the suppressive effect of UC-MSCs on the proliferation, invasive behavior and inflammatory responses of FLSs from RA patients. We also demonstrated that UC-MSCs could inhibit activation of T cells and induced Tregs expression in RA. More importantly, in mice, systemic infusion of UC-MSCs significantly reduced the severity of collagen-induced arthritis (CIA). In addition, the possible mechanism(s) underlying the UC-MSCs-mediated inhibitory effect were explored.
Bačenkov, Darina; Trebuňová, Marianna; Morochovič, Radoslav; Dosedla, Erik; Balogová, Alena Findrik
Interaction between Mesenchymal Stem Cells and the Immune System in Rheumatoid Arthritis Journal Article
In: 2022.
@article{nokey,
title = {Interaction between Mesenchymal Stem Cells and the Immune System in Rheumatoid Arthritis},
author = {Darina Bačenkov and Marianna Trebuňová and Radoslav Morochovič and Erik Dosedla and Alena Findrik Balogová},
url = {https://doi.org/10.3390%2Fph15080941},
year = {2022},
date = {2022-08-15},
urldate = {2022-08-15},
abstract = {Rheumatoid arthritis (RA) is an autoimmune disease that causes damage to joints. This review focuses on the possibility of influencing the disease through immunomodulation by mesenchymal stem cells (MSCs). There is an occurrence of rheumatoid factor and RA-specific autoantibodies to citrullinated proteins in most patients. Citrulline proteins have been identified in the joints of RA patients, and are considered to be the most suitable candidates for the stimulation of anti-citrulline protein antibodies production. Fibroblast-like proliferating active synoviocytes actively promote inflammation and destruction in the RA joint, in association with pro-inflammatory cells. The inflammatory process may be suppressed by MSCs, which are a population of adherent cells with the following characteristic phenotype: CD105+, CD73+, CD90+, CD45−, CD34− and HLA DR−. Following the stimulation process, MSCs are capable of immunomodulatory action through the release of bioactive molecules, as well as direct contact with the cells of the immune system. Furthermore, MSCs show the ability to suppress natural killer cell activation and dendritic cells maturation, inhibit T cell proliferation and function, and induce T regulatory cell formation. MSCs produce factors that suppress inflammatory processes, such as PGE2, TGF-β, HLA-G5, IDO, and IL-10. These properties suggest that MSCs may affect and suppress the excessive inflammation that occurs in RA. The effect of MSCs on rheumatoid arthritis has been proven to be a suitable alternative treatment thanks to successful experiments and clinical studies.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Zeng, Liuting; Yu, Ganpeng; Yang, Kailin; Xiang, Wang; Li, Jun; Chen, Hua
Efficacy and Safety of Mesenchymal Stem Cell Transplantation in the Treatment of Autoimmune Disease Journal Article
In: 2022.
@article{nokey,
title = {Efficacy and Safety of Mesenchymal Stem Cell Transplantation in the Treatment of Autoimmune Disease},
author = {Liuting Zeng and Ganpeng Yu and Kailin Yang and Wang Xiang and Jun Li and Hua Chen},
url = {https://doi.org/10.1155%2F2022%2F9463314},
year = {2022},
date = {2022-03-24},
urldate = {2022-03-24},
abstract = {Autoimmune diseases are a series of diseases caused by the immune system's response to self-antigens, resulting in self-tissue damage or dysfunction. It mainly includes systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), Sjogren's syndrome, polymyositis and dermatomyositis. Many autoimmune diseases are characterized by the production of autoantibodies, which bind to the host's own proteins or form immune complexes and deposit in tissues. Any organ of the body may become a target organ for autoimmunity, including skin, joints, kidneys, and blood vessels. The inflammatory effect caused by autoantibodies is mediated by binding to Fc receptors on leukocytes, which is an important cause of downstream tissue damage. Meanwhile, autoantibodies can also directly mediate tissue damage in diseases through complement activation [5]. In the development stage of the disease, genetic factors and environmental factors may interact in turn to promote the development of autoimmunity and ultimately lead to tissue inflammation and damage, becoming a chronic disease with multiple organs and multiple system damage.
Clinically, once diagnosed, patients should be treated with medication in time to avoid further development of the disease causing damage to organs or systems such as the liver and kidney. Clinically, commonly used glucocorticoids and traditional disease-improving antirheumatic drugs (DMARDs) have good anti-inflammatory, pain-relieving, and improving or delaying disease progression effects and are still used as the first-line choice for clinical treatment of rheumatic immune diseases [9, 10]. However, for first-line treatments with single or combined regimens that do not respond well or cannot tolerate them, other treatment options with potential curative effects need to be considered . For example, stem cell transplantation, biological preparations, or new botanical preparations, as well as some antirheumatic drug candidates that may modulate or suppress immunity, in order to alleviate the condition of patients with refractory rheumatism and improve their quality of life. Among them, mesenchymal stem cells are one of the most promising therapeutic strategies },
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Clinically, once diagnosed, patients should be treated with medication in time to avoid further development of the disease causing damage to organs or systems such as the liver and kidney. Clinically, commonly used glucocorticoids and traditional disease-improving antirheumatic drugs (DMARDs) have good anti-inflammatory, pain-relieving, and improving or delaying disease progression effects and are still used as the first-line choice for clinical treatment of rheumatic immune diseases [9, 10]. However, for first-line treatments with single or combined regimens that do not respond well or cannot tolerate them, other treatment options with potential curative effects need to be considered . For example, stem cell transplantation, biological preparations, or new botanical preparations, as well as some antirheumatic drug candidates that may modulate or suppress immunity, in order to alleviate the condition of patients with refractory rheumatism and improve their quality of life. Among them, mesenchymal stem cells are one of the most promising therapeutic strategies
González, Lina María; Ospina, Laura Natalia; Sperling, Laura Elena; Chaparro, Orlando; Cucarián, Jaison Daniel
Therapeutic Effects of Physical Exercise and the Mesenchymal Stem Cell Secretome by Modulating Neuroinflammatory Response in Multiple Sclerosis Journal Article
In: 2022.
@article{nokey,
title = {Therapeutic Effects of Physical Exercise and the Mesenchymal Stem Cell Secretome by Modulating Neuroinflammatory Response in Multiple Sclerosis},
author = {Lina María González and Laura Natalia Ospina and Laura Elena Sperling and Orlando Chaparro and Jaison Daniel Cucarián},
url = {10.2174/1574888X16666211209155333},
year = {2022},
date = {2022-02-18},
abstract = {Multiple Sclerosis (MS) is a neurodegenerative, demyelinating, and chronic inflammatory disease characterized by Central Nervous System (CNS) lesions that lead to high levels of disability and severe physical and cognitive disturbances. Conventional therapies are not enough to control the neuroinflammatory process in MS and are not able to inhibit ongoing damage to the CNS. Thus, the secretome of mesenchymal stem cells (MSC-S) has been postulated as a potential therapy that could mitigate symptoms and disease progression. We considered that its combination with physical exercise (EX) could induce superior effects and increase the MSC-S effectiveness in this condition. Recent studies have revealed that both EX and MSC-S share similar mechanisms of action that mitigate auto-reactive T cell infiltration, regulate the local inflammatory response, modulate the proinflammatory profile of glial cells, and reduce neuronal damage. Clinical and experimental studies have reported that these treatments in an isolated way also improve myelination, regeneration, promote the release of neurotrophic factors, and increase the recruitment of endogenous stem cells. Together, these effects reduce disease progression and improve patient functionality. Despite these results, the combination of these methods has not yet been studied in MS. In this review, we focus on molecular elements and cellular responses induced by these treatments in a separate way, showing their beneficial effects in the control of symptoms and disease progression in MS, as well as indicating their contribution in clinical fields. In addition, we propose the combined use of EX and MSC-S as a strategy to boost their reparative and immunomodulatory effects in this condition, combining their benefits on synaptogenesis, neurogenesis, remyelination, and neuroinflammatory response. The findings here reported are based on the scientific evidence and our professional experience that will bring significant progress to regenerative medicine to deal with this condition.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Sarsenova, Madina; Issabekova, Assel; Abisheva, Saule; Rutskaya-Moroshan, Kristina; Ogay, Vyacheslav; Saparov, Arman
Mesenchymal Stem Cell-Based Therapy for Rheumatoid Arthritis Journal Article
In: 2021.
@article{nokey,
title = {Mesenchymal Stem Cell-Based Therapy for Rheumatoid Arthritis},
author = {Madina Sarsenova and Assel Issabekova and Saule Abisheva and Kristina Rutskaya-Moroshan and Vyacheslav Ogay and Arman Saparov},
url = {https://doi.org/10.3390%2Fijms222111592},
year = {2021},
date = {2021-11-22},
abstract = {Mesenchymal stem cells (MSCs) have great potential to differentiate into various types of cells, including but not limited to, adipocytes, chondrocytes and osteoblasts. In addition to their progenitor characteristics, MSCs hold unique immunomodulatory properties that provide new opportunities in the treatment of autoimmune diseases, and can serve as a promising tool in stem cell-based therapy. Rheumatoid arthritis (RA) is a chronic systemic autoimmune disorder that deteriorates quality and function of the synovium membrane, resulting in chronic inflammation, pain and progressive cartilage and bone destruction. The mechanism of RA pathogenesis is associated with dysregulation of innate and adaptive immunity. Current conventional treatments by steroid drugs, antirheumatic drugs and biological agents are being applied in clinical practice. However, long-term use of these drugs causes side effects, and some RA patients may acquire resistance to these drugs. In this regard, recently investigated MSC-based therapy is considered as a promising approach in RA treatment. In this study, we review conventional and modern treatment approaches, such as MSC-based therapy through the understanding of the link between MSCs and the innate and adaptive immune systems. Moreover, we discuss recent achievements in preclinical and clinical studies as well as various strategies for the enhancement of MSC immunoregulatory properties.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Shen, Ziwei; Huang, Wei; Liu, Jun; Tian, Jie; Wang, Shengjun; Rui, Ke
Effects of Mesenchymal Stem Cell-Derived Exosomes on Autoimmune Diseases Journal Article
In: 2021.
@article{nokey,
title = {Effects of Mesenchymal Stem Cell-Derived Exosomes on Autoimmune Diseases},
author = {Ziwei Shen and Wei Huang and Jun Liu and Jie Tian and Shengjun Wang and Ke Rui},
url = {https://doi.org/10.3389/fimmu.2021.749192},
year = {2021},
date = {2021-09-21},
urldate = {2021-09-21},
abstract = {Recent years, the immunosuppressive properties of mesenchymal stem cells (MSCs) have been demonstrated in preclinical studies and trials of inflammatory and autoimmune diseases. Emerging evidence indicates that the immunomodulatory effect of MSCs is primarily attributed to the paracrine pathway. As one of the key paracrine effectors, mesenchymal stem cell-derived exosomes (MSC-EXOs) are small vesicles 30-200 nm in diameter that play an important role in cell-to-cell communication by carrying bioactive substances from parental cells. Recent studies support the finding that MSC-EXOs have an obvious inhibitory effect toward different effector cells involved in the innate and adaptive immune response. Moreover, substantial progress has been made in the treatment of autoimmune diseases, including multiple sclerosis (MS), systemic lupus erythematosus (SLE), type-1 diabetes (T1DM), uveitis, rheumatoid arthritis (RA), and inflammatory bowel disease (IBD). MSC-EXOs are capable of reproducing MSC function and overcoming the limitations of traditional cell therapy. Therefore, using MSC-EXOs instead of MSCs to treat autoimmune diseases appears to be a promising cell-free treatment strategy. In this review, we review the current understanding of MSC-EXOs and discuss the regulatory role of MSC-EXOs on immune cells and its potential application in autoimmune diseases.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Hwang, Joel Jihwan; Rim, Yeri Alice; Nam, Yoojun; Ju, Ji Hyeon
Recent Developments in Clinical Applications of Mesenchymal Stem Cells in the Treatment of Rheumatoid Arthritis and Osteoarthritis Journal Article
In: 2021.
@article{nokey,
title = {Recent Developments in Clinical Applications of Mesenchymal Stem Cells in the Treatment of Rheumatoid Arthritis and Osteoarthritis},
author = {Joel Jihwan Hwang and Yeri Alice Rim and Yoojun Nam and Ji Hyeon Ju},
url = {https://doi.org/10.3389%2Ffimmu.2021.631291},
year = {2021},
date = {2021-03-08},
urldate = {2021-03-08},
abstract = {Mesenchymal stem cell (MSC) therapies have been used as cell-based treatments for decades, owing to their anti-inflammatory, immunomodulatory, and regenerative properties. With high expectations, many ongoing clinical trials are investigating the safety and efficacy of MSC therapies to treat arthritic diseases. Studies on osteoarthritis (OA) have shown positive clinical outcomes, with improved joint function, pain level, and quality of life. In addition, few clinical MSC trials conducted on rheumatoid arthritis (RA) patients have also displayed some optimistic outlook. The largely positive outcomes in clinical trials without severe side effects establish MSCs as promising tools for arthritis treatment. However, further research is required to investigate its applicability in clinical settings. This review discusses the most recent advances in clinical studies on MSC therapies for OA and RA.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
El-Jawhari, Jehan J.; El-Sherbiny, Yasser; McGonagle, Dennis; Jones, Elena
In: 2021.
@article{nokey,
title = {Multipotent Mesenchymal Stromal Cells in Rheumatoid Arthritis and Systemic Lupus Erythematosus; From a Leading Role in Pathogenesis to Potential Therapeutic Saviors?},
author = {Jehan J. El-Jawhari and Yasser El-Sherbiny and Dennis McGonagle and Elena Jones},
url = {https://doi.org/10.3389%2Ffimmu.2021.643170},
year = {2021},
date = {2021-02-24},
urldate = {2021-02-24},
abstract = {The pathogenesis of the autoimmune rheumatological diseases including rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) is complex with the involvement of several immune cell populations spanning both innate and adaptive immunity including different T-lymphocyte subsets and monocyte/macrophage lineage cells. Despite therapeutic advances in RA and SLE, some patients have persistent and stubbornly refractory disease. Herein, we discuss stromal cells' dual role, including multipotent mesenchymal stromal cells (MSCs) also used to be known as mesenchymal stem cells as potential protagonists in RA and SLE pathology and as potential therapeutic vehicles. Joint MSCs from different niches may exhibit prominent pro-inflammatory effects in experimental RA models directly contributing to cartilage damage. These stromal cells may also be key regulators of the immune system in SLE. Despite these pro-inflammatory roles, MSCs may be immunomodulatory and have potential therapeutic value to modulate immune responses favorably in these autoimmune conditions. In this review, the complex role and interactions between MSCs and the haematopoietically derived immune cells in RA and SLE are discussed. The harnessing of MSC immunomodulatory effects by contact-dependent and independent mechanisms, including MSC secretome and extracellular vesicles, is discussed in relation to RA and SLE considering the stromal immune microenvironment in the diseased joints. Data from translational studies employing MSC infusion therapy against inflammation in other settings are contextualized relative to the rheumatological setting. Although safety and proof of concept studies exist in RA and SLE supporting experimental and laboratory data, robust phase 3 clinical trial data in therapy-resistant RA and SLE is still lacking.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Petrou, Panayiota; Kassis, Ibrahim; Levin, Netta; Paul, Friedemann; Backner, Yael; Benoliel, Tal; Oertel, Frederike Cosima
Beneficial effects of autologous mesenchymal stem cell transplantation in active progressive multiple sclerosis Journal Article
In: 2020.
@article{nokey,
title = {Beneficial effects of autologous mesenchymal stem cell transplantation in active progressive multiple sclerosis},
author = {Panayiota Petrou and Ibrahim Kassis and Netta Levin and Friedemann Paul and Yael Backner and Tal Benoliel and Frederike Cosima Oertel},
url = {https://doi.org/10.1093/brain/awaa333},
year = {2020},
date = {2020-12-01},
urldate = {2020-12-01},
abstract = {In this study (trial registration: NCT02166021), we aimed to evaluate the optimal way of administration, the safety and the clinical efficacy of mesenchymal stem cell (MSC) transplantation in patients with active and progressive multiple sclerosis. Forty-eight patients (28 males and 20 females) with progressive multiple sclerosis (Expanded Disability Status Scale: 3.0-6.5, mean : 5.6 ± 0.8, mean age: 47.5 ± 12.3) and evidence of either clinical worsening or activity during the previous year, were enrolled (between 2015 and 2018). Patients were randomized into three groups and treated intrathecally (IT) or intravenously (IV) with autologous MSCs (1 × 106/kg) or sham injections. After 6 months, half of the patients from the MSC-IT and MSC-IV groups were retreated with MSCs, and the other half with sham injections. Patients initially assigned to sham treatment were divided into two subgroups and treated with either MSC-IT or MSC-IV. The study duration was 14 months. No serious treatment-related safety issues were detected. Significantly fewer patients experienced treatment failure in the MSC-IT and MSC-IV groups compared with those in the sham-treated group (6.7%, 9.7%, and 41.9%, respectively, P = 0.0003 and P = 0.0008). During the 1-year follow-up, 58.6% and 40.6% of patients treated with MSC-IT and MSC-IV, respectively, exhibited no evidence of disease activity compared with 9.7% in the sham-treated group (P < 0.0001 and P < 0.0048, respectively). MSC-IT transplantation induced additional benefits on the relapse rate, on the monthly changes of the T2 lesion load on MRI, and on the timed 25-foot walking test, 9-hole peg test, optical coherence tomography, functional MRI and cognitive tests. Treatment with MSCs was well-tolerated in progressive multiple sclerosis and induced short-term beneficial effects regarding the primary end points, especially in the patients with active disease. The intrathecal administration was more efficacious than the intravenous in several parameters of the disease. A phase III trial is warranted to confirm these findings.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Lopez-Santalla, Mercedes; Fernandez-Perez, Raquel; Garin, Marina I.
Mesenchymal Stem/Stromal Cells for Rheumatoid Arthritis Treatment: An Update on Clinical Applications Journal Article
In: 2020.
@article{nokey,
title = {Mesenchymal Stem/Stromal Cells for Rheumatoid Arthritis Treatment: An Update on Clinical Applications},
author = {Mercedes Lopez-Santalla and Raquel Fernandez-Perez and Marina I. Garin},
url = {https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7465092/#:~:text=10.3390/cells9081852},
year = {2020},
date = {2020-08-09},
abstract = {Rheumatoid arthritis (RA) is a chronic systemic autoimmune disease that affects the lining of the synovial joints leading to stiffness, pain, inflammation, loss of mobility, and erosion of joints. Its pathogenesis is related to aberrant immune responses against the synovium. Dysfunction of innate and adaptive immunity, including dysregulated cytokine networks and immune complex-mediated complement activation, are involved in the progression of RA. At present, drug treatments, including corticosteroids, antirheumatic drugs, and biological agents, are used in order to modulate the altered immune responses. Chronic use of these drugs may cause adverse effects to a significant number of RA patients. Additionally, some RA patients are resistant to these therapies. In recent years, mesenchymal stem/stromal cell (MSCs)-based therapies have been largely proposed as a novel and promising stem cell therapeutic approach in the treatment of RA. MSCs are multipotent progenitor cells that have immunomodulatory properties and can be obtained and expanded easily. Today, nearly one hundred studies in preclinical models of RA have shown promising trends for clinical application. Proof-of-concept clinical studies have demonstrated satisfactory safety profile of MSC therapy in RA patients. The present review discusses MSC-based therapy approaches with a focus on published clinical data, as well as on clinical trials, for treatment of RA that are currently underway.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Wang, Liming; Huang, Shigao; Li, Shimei; Li, Ming; Shi, Jun; Bai, Wen; Wang, Qianyun; Zheng, Libo; Liu, Yongjun
Efficacy and Safety of Umbilical Cord Mesenchymal Stem Cell Therapy for Rheumatoid Arthritis Patients: A Prospective Phase I/II Study Journal Article
In: 2019.
@article{nokey,
title = {Efficacy and Safety of Umbilical Cord Mesenchymal Stem Cell Therapy for Rheumatoid Arthritis Patients: A Prospective Phase I/II Study},
author = {Liming Wang and Shigao Huang and Shimei Li and Ming Li and Jun Shi and Wen Bai and Qianyun Wang and Libo Zheng and Yongjun Liu},
url = {https://doi.org/10.2147%2FDDDT.S225613},
year = {2019},
date = {2019-12-19},
urldate = {2019-12-19},
abstract = {Rheumatoid arthritis (RA) is a chronic, autoimmune disease affecting multiple joints symmetrically.1 The main symptoms at the early stage of the disease are joint pain and swelling; at late stage, arthritis leads to joint stiffness, malformation, loss of function, and even disability.2 Currently, available medication for RA treatment has limited efficacy, including non-steroidal anti-inflammatory drugs (NSAIDs), disease-modifying anti-rheumatic drugs (DMARDs) and immunosuppressants.3 The target cytokine therapy has some therapeutic effects but without significant repair of injured joints, which restricts its widespread clinical use.
Mesenchymal stem cells (MSCs) are characterized by their regenerative property to repair parenchymal tissue and organs through differentiating into lineages of mesenchymal tissues, as well as immunomodulation.4 Injected MSCs can migrate to injured tissues and facilitate the recovery of damaged cells.5 Clinical studies have demonstrated the clinical benefits of MSCs in RA therapy.6 However, the therapeutic benefits of umbilical cord tissue-derived MSCs (UC-MSCs) for the treatment of RA have not been well studied clinically. As is known that the key factor in the pathogenesis of RA is the elevated cytokines arising from numerous synovial cells.7 MSCs can express various receptors for pro-inflammatory cytokines8 to reduce inflammation in RA patients. We have previously reported the safety and efficacy of UC-MSC for the treatment of RA patients for up to 8 months after UC-MSC infusion.9 The aim of this 3-year cohort study is to assess the long-term efficacy and safety of UC-MSC plus DMARDs therapy for RA. The data demonstrated that UC-MSC treatment was safe and able to benefit RA patients in long term when combined with DMARDs. Continuous UC-MSC treatment can resume patients’ physical activity function to achieve excellent clinical benefits.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Mesenchymal stem cells (MSCs) are characterized by their regenerative property to repair parenchymal tissue and organs through differentiating into lineages of mesenchymal tissues, as well as immunomodulation.4 Injected MSCs can migrate to injured tissues and facilitate the recovery of damaged cells.5 Clinical studies have demonstrated the clinical benefits of MSCs in RA therapy.6 However, the therapeutic benefits of umbilical cord tissue-derived MSCs (UC-MSCs) for the treatment of RA have not been well studied clinically. As is known that the key factor in the pathogenesis of RA is the elevated cytokines arising from numerous synovial cells.7 MSCs can express various receptors for pro-inflammatory cytokines8 to reduce inflammation in RA patients. We have previously reported the safety and efficacy of UC-MSC for the treatment of RA patients for up to 8 months after UC-MSC infusion.9 The aim of this 3-year cohort study is to assess the long-term efficacy and safety of UC-MSC plus DMARDs therapy for RA. The data demonstrated that UC-MSC treatment was safe and able to benefit RA patients in long term when combined with DMARDs. Continuous UC-MSC treatment can resume patients’ physical activity function to achieve excellent clinical benefits.
Genc, Bilgesu; Bozan, Hemdem Rodi; Genc, Sermin; Genc, Kursad
Stem Cell Therapy for Multiple Sclerosis Journal Article
In: 2018.
@article{nokey,
title = {Stem Cell Therapy for Multiple Sclerosis},
author = {Bilgesu Genc and Hemdem Rodi Bozan and Sermin Genc and Kursad Genc},
url = {https://dx.doi.org/10.1007/5584_2018_247},
year = {2018},
date = {2018-07-24},
abstract = {Multiple sclerosis (MS) is a chronic inflammatory, autoimmune, and neurodegenerative disease of the central nervous system (CNS). It is characterized by demyelination and neuronal loss that is induced by attack of autoreactive T cells to the myelin sheath and endogenous remyelination failure, eventually leading to functional neurological disability. Although recent evidence suggests that MS relapses are induced by environmental and exogenous triggers such as viral infections in a genetic background, its very complex pathogenesis is not completely understood. Therefore, the efficiency of current immunosuppression-based therapies of MS is too low, and emerging disease-modifying immunomodulatory agents such as fingolimod and dimethyl fumarate cannot stop progressive neurodegenerative process. Thus, the cell replacement therapy approach that aims to overcome neuronal cell loss and remyelination failure and to increase endogenous myelin repair capacity is considered as an alternative treatment option. A wide variety of preclinical studies, using experimental autoimmune encephalomyelitis model of MS, have recently shown that grafted cells with different origins including mesenchymal stem cells (MSCs), neural precursor and stem cells, and induced-pluripotent stem cells have the ability to repair CNS lesions and to recover functional neurological deficits. The results of ongoing autologous hematopoietic stem cell therapy studies, with the advantage of peripheral administration to the patients, have suggested that cell replacement therapy is also a feasible option for immunomodulatory treatment of MS. In this chapter, we overview cell sources and applications of the stem cell therapy for treatment of MS. We also discuss challenges including those associated with administration route, immune responses to grafted cells, integration of these cells to existing neural circuits, and risk of tumor growth. Finally, future prospects of stem cell therapy for MS are addressed.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Franceschetti, Tiziana; Bari, Cosimo De
The potential role of adult stem cells in the management of the rheumatic diseases Journal Article
In: 2017.
@article{nokey,
title = {The potential role of adult stem cells in the management of the rheumatic diseases},
author = {Tiziana Franceschetti and Cosimo De Bari},
url = {https://doi.org/10.1177%2F1759720X17704639},
year = {2017},
date = {2017-04-20},
urldate = {2017-04-20},
abstract = {Adult stem cells are considered as appealing therapeutic candidates for inflammatory and degenerative musculoskeletal diseases. A large body of preclinical research has contributed to describing their immune-modulating properties and regenerative potential. Additionally, increasing evidence suggests that stem cell differentiation and function are disrupted in the pathogenesis of rheumatic diseases. Clinical studies have been limited, for the most part, to the application of adult stem cell-based treatments on small numbers of patients or as a ‘salvage’ therapy in life-threatening disease cases. Nevertheless, these preliminary studies indicate that adult stem cells are promising tools for the long-term treatment of rheumatic diseases. This review highlights recent knowledge acquired in the fields of hematopoietic and mesenchymal stem cell therapy for the management of systemic sclerosis (SSc), systemic lupus erythematosus (SLE), rheumatoid arthritis (RA) and osteoarthritis (OA) and the potential mechanisms mediating their function.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Ennis, William J.; Sui, Audrey; Bartholomew, Amelia
Stem Cells and Healing: Impact on Inflammation Journal Article
In: 2013.
@article{nokey,
title = {Stem Cells and Healing: Impact on Inflammation},
author = {William J. Ennis and Audrey Sui and Amelia Bartholomew},
url = {https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3842880/},
year = {2013},
date = {2013-09-02},
abstract = {Significance
The number of patients with nonhealing wounds has rapidly accelerated over the past 10 years in both the United States and worldwide. Some causative factors at the macro level include an aging population, epidemic numbers of obese and diabetic patients, and an increasing number of surgical procedures. At the micro level, chronic inflammation is a consistent finding.
Recent Advances
A number of treatment modalities are currently used to accelerate wound healing, including energy-based modalities, scaffoldings, the use of mechano-transduction, cytokines/growth factors, and cell-based therapies. The use of stem cell therapy has been hypothesized as a potentially useful adjunct for nonhealing wounds. Specifically, mesenchymal stem cells (MSCs) have been shown to improve wound healing in several studies. Immune modulating properties of MSCs have made them attractive treatment options.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
The number of patients with nonhealing wounds has rapidly accelerated over the past 10 years in both the United States and worldwide. Some causative factors at the macro level include an aging population, epidemic numbers of obese and diabetic patients, and an increasing number of surgical procedures. At the micro level, chronic inflammation is a consistent finding.
Recent Advances
A number of treatment modalities are currently used to accelerate wound healing, including energy-based modalities, scaffoldings, the use of mechano-transduction, cytokines/growth factors, and cell-based therapies. The use of stem cell therapy has been hypothesized as a potentially useful adjunct for nonhealing wounds. Specifically, mesenchymal stem cells (MSCs) have been shown to improve wound healing in several studies. Immune modulating properties of MSCs have made them attractive treatment options.
Lihua Wang Liming Wang, Xiuli Cong
Human umbilical cord mesenchymal stem cell therapy for patients with active rheumatoid arthritis: safety and efficacy Journal Article
In: 2013.
@article{,
title = {Human umbilical cord mesenchymal stem cell therapy for patients with active rheumatoid arthritis: safety and efficacy},
author = {Liming Wang , Lihua Wang, Xiuli Cong, Guangyang Liu, Jianjun Zhou, Bin Bai, Yang Li, Wen Bai, Ming Li, Haijie Ji, Delin Zhu, Mingyuan Wu, Yongjun Liu},
url = {https://doi.org/10.1089/scd.2013.0023},
year = {2013},
date = {2013-08-13},
urldate = {2013-08-13},
abstract = {This study was designed to assess the safety and efficacy of human umbilical cord mesenchymal stem cells (UC-MSCs) in the treatment of rheumatoid arthritis (RA). In this ongoing cohort, 172 patients with active RA who had inadequate responses to traditional medication were enrolled. Patients were divided into two groups for different treatment: disease-modifying anti-rheumatic drugs (DMARDs) plus medium without UC-MSCs, or DMARDs plus UC-MSCs group (4×107 cells per time) via intravenous injection. Adverse events and the clinical information were recorded. Tests for serological markers to assess safety and disease activity were conducted. Serum levels of inflammatory chemokines/cytokines were measured, and lymphocyte subsets in peripheral blood were analyzed. No serious adverse effects were observed during or after infusion. The serum levels of tumor necrosis factor-alpha and interleukin-6 decreased after the first UC-MSCs treatment (P<0.05). The percentage of CD4+CD25+Foxp3+ regulatory T cells of peripheral blood was increased (P<0.05). The treatment induced a significant remission of disease according to the American College of Rheumatology improvement criteria, the 28-joint disease activity score, and the Health Assessment Questionnaire. The therapeutic effects maintained for 3–6 months without continuous administration, correlating with the increased percentage of regulatory T cells of peripheral blood. Repeated infusion after this period can enhance the therapeutic efficacy. In comparison, there were no such benefits observed in control group of DMARDS plus medium without UC-MSCs. Thus, our data indicate that treatment with DMARDs plus UC-MSCs may provide safe, significant, and persistent clinical benefits for patients with active RA.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
Liu, Yanying; Mu, Rong; Wang, Shiyao; Long,; Liu, Xia
Therapeutic potential of human umbilical cord mesenchymal stem cells in the treatment of rheumatoid arthritis Journal Article
In: 2010.
@article{nokey,
title = {Therapeutic potential of human umbilical cord mesenchymal stem cells in the treatment of rheumatoid arthritis},
author = {Yanying Liu and Rong Mu and Shiyao Wang and Long and Xia Liu},
url = {https://doi.org/10.1186%2Far3187},
year = {2010},
date = {2010-11-16},
urldate = {2010-11-16},
abstract = {Rheumatoid arthritis (RA) is a chronic and systemic disease that primarily attacks synovial joints, leading to articular destruction and functional disability. RA imparts a massive burden on health services worldwide. Efforts to discover new target therapies have achieved considerable success. For instance, TNF-α inhibitors and B-cell-depleting therapies have benefited many RA patients [1,2]. However, these approaches are expensive and none of the currently widely used biological agents reaches longterm drug-free remission [3,4]. Therefore, it is important to develop new and more effective therapy for RA.
In RA, proinflammatory cytokines, such as TNF-α, IL-6, IL-1β and IL-17, play dominant pathological roles. Aberrant T help cells (Th) 17 and Th1 responses have been linked to pathogenesis of RA [5-7]. Furthermore, evidence is accumulating that a defect in number or function of regular T cells (Tregs) is important in the immune imbalance that culminates in RA [8,9]. The fibroblast-like synoviocytes (FLSs) are resident cells of synovial joints, involved in pannus formation, and are key players in the destruction of cartilage and bone in RA joint [10]. The ability of FLSs to stimulate both inflammation and tissue damage suggests that this cell type may be another critical target for the treatment of inflammatory arthritis [11].
Mesenchymal stem cells (MSCs) are cells of stromal origin that can exert profound immunosuppression by modulating T and B cell proliferation and differentiation, dendritic cell maturation and NK activity. These immunoregulatory properties encouraged a possible use of these cells to modulate autoimmune responses and in the treatment of autoimmue diseases [12,13]. To date, the experience of MSCs in the treatment of RA is limited to a few cases, with controversial results from preclinical models [14-18]. As of yet, the most common source of MSCs has been bone marrow. However, aspirating bone marrow is an invasive procedure. In addition, the number and the differentiating potential of bone marrow MSCs (BM-MSCs) decrease with age [19,20]. In contrast, the umbilical cord is a postnatal organ discarded after birth. The collection of umbilical cord MSCs (UC-MSCs) does not require any invasive procedure. In addition to the well-documented self-renewal and multipotent differentiation properties, UC-MSCs possess immunoregulatory capacities that have been permissive to allogeneic transplantation [21]. Given these characteristics, particularly the plasticity and developmental flexibility, the UC-MSCs are now considered an alternative source of stem cells and deserve to be examined in long-term clinical trials [22]. However, very little is known about UC-MSCs, and of note, there has been no report about UC-MSCs in the treatment of RA.
In this study, we reported our findings of the suppressive effect of UC-MSCs on the proliferation, invasive behavior and inflammatory responses of FLSs from RA patients. We also demonstrated that UC-MSCs could inhibit activation of T cells and induced Tregs expression in RA. More importantly, in mice, systemic infusion of UC-MSCs significantly reduced the severity of collagen-induced arthritis (CIA). In addition, the possible mechanism(s) underlying the UC-MSCs-mediated inhibitory effect were explored.},
keywords = {},
pubstate = {published},
tppubtype = {article}
}
In RA, proinflammatory cytokines, such as TNF-α, IL-6, IL-1β and IL-17, play dominant pathological roles. Aberrant T help cells (Th) 17 and Th1 responses have been linked to pathogenesis of RA [5-7]. Furthermore, evidence is accumulating that a defect in number or function of regular T cells (Tregs) is important in the immune imbalance that culminates in RA [8,9]. The fibroblast-like synoviocytes (FLSs) are resident cells of synovial joints, involved in pannus formation, and are key players in the destruction of cartilage and bone in RA joint [10]. The ability of FLSs to stimulate both inflammation and tissue damage suggests that this cell type may be another critical target for the treatment of inflammatory arthritis [11].
Mesenchymal stem cells (MSCs) are cells of stromal origin that can exert profound immunosuppression by modulating T and B cell proliferation and differentiation, dendritic cell maturation and NK activity. These immunoregulatory properties encouraged a possible use of these cells to modulate autoimmune responses and in the treatment of autoimmue diseases [12,13]. To date, the experience of MSCs in the treatment of RA is limited to a few cases, with controversial results from preclinical models [14-18]. As of yet, the most common source of MSCs has been bone marrow. However, aspirating bone marrow is an invasive procedure. In addition, the number and the differentiating potential of bone marrow MSCs (BM-MSCs) decrease with age [19,20]. In contrast, the umbilical cord is a postnatal organ discarded after birth. The collection of umbilical cord MSCs (UC-MSCs) does not require any invasive procedure. In addition to the well-documented self-renewal and multipotent differentiation properties, UC-MSCs possess immunoregulatory capacities that have been permissive to allogeneic transplantation [21]. Given these characteristics, particularly the plasticity and developmental flexibility, the UC-MSCs are now considered an alternative source of stem cells and deserve to be examined in long-term clinical trials [22]. However, very little is known about UC-MSCs, and of note, there has been no report about UC-MSCs in the treatment of RA.
In this study, we reported our findings of the suppressive effect of UC-MSCs on the proliferation, invasive behavior and inflammatory responses of FLSs from RA patients. We also demonstrated that UC-MSCs could inhibit activation of T cells and induced Tregs expression in RA. More importantly, in mice, systemic infusion of UC-MSCs significantly reduced the severity of collagen-induced arthritis (CIA). In addition, the possible mechanism(s) underlying the UC-MSCs-mediated inhibitory effect were explored.

Omni-Stem Cell-based Therapies
Umbilical cord mesenchymal stem cell therapies utilize the capabilities of stem cells and their exosomes to modulate the immune system, reduce inflammation, and support tissue repair. While these therapies show considerable promise, clinical evidence highlights that the therapeutic potential and safety profiles of regenerative medicine in treating autoimmune disorders.
Contact us to schedule an online consultation
Complete the form to speak with our patient advocates and learn more about Omni-Stem cell-based treatments.

DISCOVER REGENERATIVE MEDICINE
Visit our resource center for a comprehensive collection of resources, studies, and recent advancements in Regenerative Medicine.
Stem cell treatments are currently deemed experimental and have not yet received FDA approval. As a result, such treatments are not permitted in the U.S. While this doesn’t imply that these treatments are ineffective, it does indicate that there’s limited scientific evidence supporting their use.
U-MSC stem cells are currently the most potent biologics available in regenerative medicine.
U-MSC stem cells are a new approach for treating autoimmune diseases, such as rheumatoid arthritis, lupus, and Crohn’s disease; Regenerative medicine potential is rooted in its ability to influence the body’s immune response.